If you’ve ever taken an over-the-counter (OTC) cold or flu tablet and wondered why your nose is still blocked, you’re not alone.
For years in Australia (and globally) many consumers have relied on oral decongestants especially those with Phenylephrine (PE) as the active ingredient, but mounting evidence suggests that these options often fail to deliver the relief patients expect.
Meanwhile, the former standard, Pseudoephedrine (PSE), which is demonstrably more effective, remains tightly regulated.
My 20+ years of experience working in the Pharmaceutical Industry has exposed my interest towards PSE-based products and their current and future development in Australia.
My discovery and interest of this revealed that this is far more than just a commercial oversight but also a public-health and regulatory opportunity.
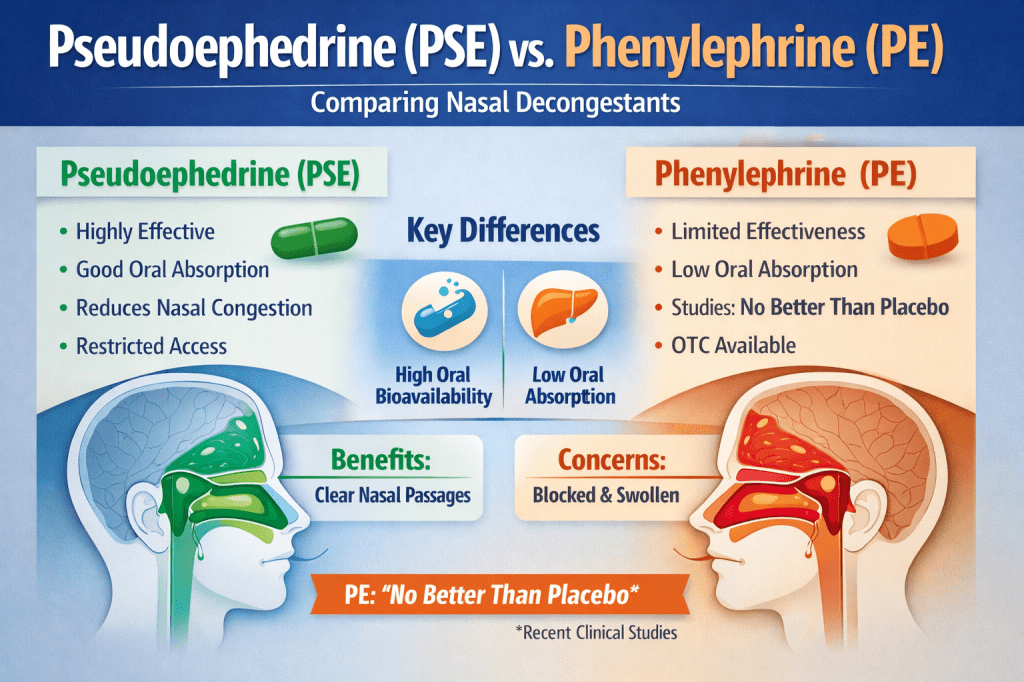
For decades, pseudoephedrine (PSE) was the mainstay oral decongestant ingredient in cold and flu medicines. It works by constricting blood vessels in the nasal passages, reducing swelling and congestion.
However, in the mid-2000s, as governments cracked down on illicit methamphetamine production, pseudoephedrine’s sale became tightly controlled.
The Clinical Effectiveness Difference: PSE vs PE
Both PSE and PE act as decongestants by stimulating α-adrenergic receptors in nasal mucosal blood vessels, causing vasoconstriction the eventuates into reducing capillary blood flow and thereby lowering mucosal swelling and congestion.
Pseudoephedrine is well-absorbed orally and has a reliable pharmacokinetic profile; hence its therapeutic effect is consistent.
By contrast, oral phenylephrine’s systemic bioavailability is dramatically reduced by hepatic first-pass metabolism, which undermines its clinical potency.
Key Clinical Studies and Reviews
- In 2006, a Letter to the Editor was published at the Journal of Allergy and Clinical Immunology in regards to PSE and PE. The letter detailed that there have been significant changes to the method for consumers to obtain PSE-based decongestants, as well as a double-blind crossover study evaluated nasal airway resistance (NAR) in 20 patients with chronic nasal stuffiness. The study found significant reductions with pseudoephedrine and phenylpropanolamine, but not with phenylephrine. [1]
- In 2009, a placebo-controlled study of the nasal decongestant effect of PE and PSE was performed in the Vienna Challenge Chamber. The study has been published in the Annals of Allergy, Asthma, and Immunology. The study involved 39 grass-allergic patients that were dosed with immediate-release formulations of phenylephrine, 12 mg, pseudoephedrine, 60 mg, as a control, or placebo. Pseudoephedrine significantly improved nasal congestion and inspiratory flow, whereas Phenylephrine did not significantly improve in measures of nasal congestion. [2]
- In 2024, there was an article published under the Cureus Journal of Medical Science called “The Use and Efficacy of Oral Phenylephrine Versus Placebo Treating Nasal Congestion Over the Years on Adults: A Systematic Review”. It concluded that the available studies for oral phenylephrine show that it is no different from placebo in treating nasal congestion. Further research may be required to determine the role of oral phenylephrine in managing nasal congestion instead. [3]
- Last year in 2025, there was an article published under European Archives of Oto-Rhino-Laryngology on “A comment on oral phenylephrine use in sinonasal pathologies” that noted that while oral PE is still popular, its lack of demonstrating efficacy with support of trials has called its use and its status as an OTC medication into question. [4]
Regulatory and pharmacokinetic context
According to the U.S. Food & Drug Administration (FDA) review, when PE is administered orally in the 10 mg dose typical of many OTC formulations, the parent drug’s bioavailability is less than 1 % (in a 14-volunteer study). [5]
The FDA’s Nonprescription Drugs Advisory Committee has raised concerns that the aliquot of active drug reaching the nasal tissues may be insufficient to produce a meaningful decongestant effect. [6]
In contrast, pseudoephedrine retains good oral bioavailability, penetrates nasal mucosa, and reliably reduces nasal airway resistance. Its adverse-event profile is well known and manageable (e.g., mild insomnia, elevated blood pressure in some patients).
What this means in Australian OTC practice?
In Australia, following tightening of pseudoephedrine access (driven by diversion risks), many companies substituted oral phenylephrine in their combination cold/flu/decongestant products.
The result, consumers may assume they are getting a clinically effective decongestant, but the evidence suggests many are not.
This mismatch creates three real consequences:
- Therapeutic dissatisfaction – Customers feel the product “doesn’t work”, undermining confidence in OTC pharmacy-care.
- Clinical inertia – Because PE is seen as safe and accessible, the impetus to push for stronger regulatory or formulary change remains low.
- Opportunity for advocacy – There is a clear case for revisiting our OTC options in Australia and aligning supply with best-available evidence, while managing safety and diversion risk.
Why now is the right time to revisit the conversation?
- Globally regulatory bodies are waking up to the efficacy gap: the FDA advisory committee in 2023 unanimously concluded that the evidence does not support that the current dosage of oral phenylephrine is effective as a nasal decongestant. [4]
- Pharmacy systems (including in Australia) now have far more robust real-time monitoring capability (e.g., electronic sales records, pharmacist oversight) than what was available when PSE was first restricted.
- Customers, pharmacists and clinicians are increasingly outcome-driven: they expect real relief, not just marketing claims.
Closing thought
It’s time to re-examine how we regulate and supply oral decongestants in Australia. Millions of Australians trust pharmacy staff for everyday relief of nasal congestion, but trust can only be preserved when what we supply actually works.
With modern monitoring tools, pharmacy practice capability and a strong evidence base for pseudoephedrine, we have the framework to balance safety and efficacy.
My view: if we ignore this gap any longer, we risk undermining OTC credibility and most importantly, we risk letting patients settle for sub-optimal relief.
References
[4] A comment on oral phenylephrine use in sinonasal pathologies
[5] What Happened to Phenylephrine?
Authors Note: Wilson Prasad also known as user name muefatiaki1966 is trying to leverage his experience working on products containing PSE in Australia for over 20 years and would like to express his interest and concern of PSE based products in Australia.

Leave a comment